Is There a Machine That Can Test Eyesight With No Input From the Patient
Authored by Dr. Pascal Sacré via GlobalResearch.ca,
It is time for everyone to come up out of this negative trance, this commonage hysteria, considering dearth, poverty, massive unemployment volition kill, mow down many more than people than SARS-CoV-two!

Introduction: using a technique to lock down society
All current propaganda on the COVID-19 pandemic is based on an supposition that is considered obvious, truthful and no longer questioned:
Positive RT-PCR examination means being sick with COVID. This assumption is misleading.
Very few people, including doctors, understand how a PCR test works.
RT-PCR waysReal Time-Polymerase ChainReaction.
In French, it ways: Réaction de Polymérisation en Chaîne en Temps Réel.
In medicine, we utilise this tool mainly to diagnose a viral infection.
Starting from a clinical state of affairs with the presence or absenteeism of particular symptoms in a patient, nosotros consider dissimilar diagnoses based on tests.
In the case of sure infections, particularly viral infections, we use the RT-PCR technique to confirm a diagnostic hypothesis suggested by a clinical picture.
We do non routinely perform RT-PCR on any patient who is overheated, coughing or has an inflammatory syndrome!
It is a laboratory, molecular biology technique of cistron amplification considering it looks for gene traces (Deoxyribonucleic acid or RNA) by amplifying them.
In add-on to medicine, other fields of awarding are genetics, research, manufacture and forensics.
The technique is carried out in aspecialized laboratory, it cannot be done in whatsoever laboratory, even a infirmary. This entails a certain cost, and a delay sometimes of several days between the sample and the issue.
Today, since the emergence of the new disease chosenCOVID-19 (COronaVIrusDisease-2019), the RT-PCR diagnostic technique is used to define positive cases, confirmed as SARS-CoV-two (coronavirus responsible for the new acute respiratory distress syndrome called COVID-xix).
These positive cases are alloyed to COVID-xix cases,some of whom are hospitalized or even admitted to intensive intendance units.
Official postulate of our managers: positive RT-PCR cases = COVID-19 patients.
This is the starting postulate, the premise of all official propaganda, which justifies all restrictive government measures: isolation, confinement, quarantine, mandatory masks, colour codes by country and travel bans, tracking, social distances in companies, stores and fifty-fifty, even more chiefly, in schools.
This misuse of RT-PCR technique is used equally a relentless and intentional strategy by some governments, supported by scientific safety councils and past the dominant media,to justify excessive measures such every bit the violation of a large number of ramble rights, the destruction of the economic system with the bankruptcy of entire active sectors of society, the degradation of living conditions for a large number of ordinary citizens, under the pretext of a pandemicbased on a number of positive RT-PCR tests, and not on a real number of patients.
Technical aspects: to better sympathise and not exist manipulated
The PCR technique was developed by chemistKary B. Mullis in 1986. Kary Mullis was awarded the Nobel Prize in Chemistry in 1993.
Although this is disputed, Kary Mullis himself is said to have criticized the involvement ofPCR equally a diagnostic tool for an infection, especially a viral one.
He stated that if PCR was a good tool for enquiry, information technology was a very bad tool in medicine, in the dispensary.
Mullis was referring to the AIDS virus (HIV retrovirus or HIV), before the COVID-19 pandemic, just this opinion on the limitation of the technique in viral infections, by its creator, cannot exist dismissed out of hand; it must be taken into account!
PCR was perfected in 1992.
As the analysis can be performed in real time, continuously, it becomesRT (Real-Time) – PCR, even more than efficient.
It tin can be washed from any molecule, including those of the living, the nucleic acids that make upwards the genes:
-
DNA (deoxyribonucleic acid)
-
RNA (Ribonucleic Acrid)
Viruses are not considered as "living" beings, they are packets of data (Deoxyribonucleic acid or RNA) forming a genome.
It is by an amplification technique (multiplication) that the molecule sought is highlighted and this point is very important.
RT-PCR is an amplification technique.
If at that place is Dna or RNA of the desired element in a sample, it is not identifiable every bit such.
This Deoxyribonucleic acid or RNA must beamplified (multiplied) a certain number of times, sometimes a very large number of times, before it can be detected. From a minute trace, up to billions of copies of a specific sample can be obtained, but this does not mean that there is all that amount in the organism being tested.
In the example of COVID-19, the element sought past RT-PCR is SARS-CoV-2, an RNA virus.
In that location areDna viruses such as Herpes and Varicella viruses.
The nearly well knownRNA viruses, in addition to coronaviruses, are Influenza, Measles, EBOLA, ZIKA viruses.
In the instance of SARS-CoV-ii, RNA virus, an additional specific footstep is required, a transcription of RNA into Deoxyribonucleic acid by means of an enzyme, Reverse Transcriptase.
This step precedes the amplification phase.
It is not thewhole virus that is identified, but sequences of its viral genome.
This does non mean that this gene sequence, a fragment of the virus, is non specific to the virus being sought, but information technology is an important nuance even so:
RT-PCR does non reveal whatsoever virus, but merely parts, specific gene sequences of the virus.
At the start of the yr, the SARS-CoV-2 genome was sequenced.
It consists of about xxx,000 base pairs. The nucleic acid (DNA-RNA), the component of the genes, is a sequence of bases. In comparison, the human genome has more than 3 billion base pairs.
Teams are continuously monitoring the evolution of the SARS-CoV-2 viral genome as it evolves, through the mutations it undergoes. Today, at that place are many variants.
Past taking a few specific genes from the SARS-CoV-2 genome, it is possible to initiate RT-PCR on a sample from the respiratory tract.
For COVID-19 disease, which has a nasopharyngeal (nose) and oropharyngeal (mouth) entry bespeak, the sample should be taken from the upper respiratory tract every bit deeply as possible in order to avoid contamination past saliva in particular.
All the people tested said that information technology is very painful.
The Gold Standard (preferred site for sampling) is thenasopharyngeal (nasal) approach, the most painful route.
If there is a contraindication to the nasal approach, or preferably to the private existence tested, depending on the official organs, the oropharyngeal arroyo (through the rima oris) is besides adequate. The exam may trigger a nausea/vomiting reflex in the individual being tested.
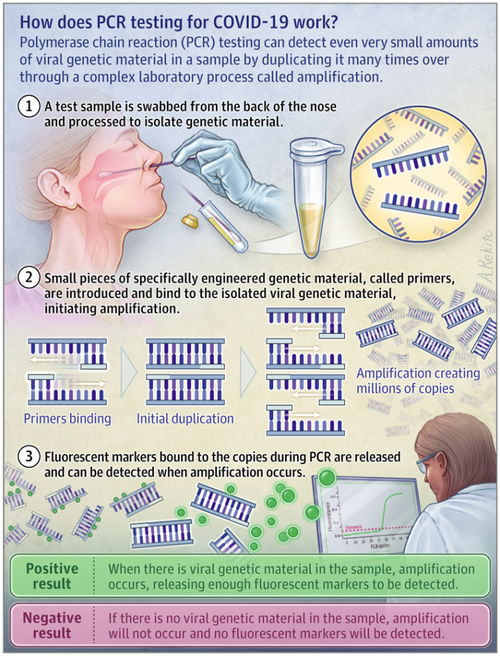
Normally, for the result of an RT-PCR test to be considered reliable,amplification from3 different genes (primers) of the virus nether investigation is required.
"The primers are unmarried-stranded Deoxyribonucleic acid sequences specific to the virus. They guarantee the specificity of the amplification reaction. »
"The commencement test adult at La Charité in Berlin past Dr. Victor Corman and his associates in January 2022 allows to highlight theRNA sequences nowadays in 3 genes of the virus called E, RdRp and North. To know if the sequences of these genes are present in the RNA samples nerveless, it is necessary to amplify the sequences of these iii genes in social club to obtain a signal sufficient for their detection and quantification. ».
The essential notion of Wheel Fourth dimension or Cycle Threshold or Ct positivity threshold [16].
An RT-PCR examination is negative (no traces of the desired element) or positive (presence of traces of the desired element).
Even so, even if the desired element is nowadays in a minute, negligible quantity, the principle of RT-PCR is to be able to finally highlight it by continuing the amplification cycles as much as necessary.
RT-PCR can push up to lx distension cycles, or even more!
Here is how it works:
-
Cycle 1: target x 2 (2 copies)
-
Bicycle 2: target x 4 (four copies)
-
Cycle iii: target x 8 (8 copies)
-
Cycle 4: target x xvi (16 copies)
-
Bike 5; target x 32 (32 copies)
-
Etc exponentially up to forty to 60 cycles!
When nosotros say that the Ct (Cycle Fourth dimension or Cycle Threshold or RT-PCR positivity threshold) is equal to 40, information technology means that the laboratory has used40 distension cycles, i.e. obtained240 copies.
This is what underlies thesensitivity of the RT-PCR analysis.
While it is true that in medicine we like to have high specificity and sensitivity of the tests to avert false positives and false negatives, in the example of COVID-19 disease, this hypersensitivity of the RT-PCR test caused by the number of amplification cycles used has backfired.
This over-sensitivity of the RT-PCR test is deleterious and misleading!
It detaches us from the medical reality which must remain based on the real clinical state of the person: is the person ill, does he or she have symptoms?
That is the nearly of import affair!
As I said at the beginning of the article, in medicine nosotros always commencement from the person: we examine him/her, nosotros collect his/her symptoms (complaints-anamnesis) and objective clinical signs (examination) and on the basis of a clinical reflection in which scientific knowledge and experience intervene, nosotros make diagnostic hypotheses.
Only so do nosotros prescribe the most appropriate tests, based on this clinical reflection.
We constantly compare the test results with the patient'southwardclinical condition (symptoms and signs), whichtakes precedence over everything else when it comes to our decisions and treatments.
Today, our governments, supported past their scientific safety communication, are making usa practise the opposite and put the test kickoff, followed past a clinical reflection necessarily influenced by this prior exam, whose weaknesses we have just seen, particularly its hypersensitivity.
None of my clinical colleagues can contradict me.
Apart from very special cases such every bit genetic screening for sure categories of populations (age groups, sexual practice) and certain cancers or family unit genetic diseases, we always work in this direction: from the person (symptoms, signs) to the appropriate tests, never the other way around.
This is the conclusion of an article in the Swiss Medical Journal (RMS) published in 2007, written past doctors Katia Jaton and Gilbert Greub microbiologists from the University of Lausanne :
PCR in microbiology: from DNA amplification to result interpretation:
"To translate the result of a PCR, it is essential that clinicians and microbiologists share their experiences, and so that the analytical and clinical levels of interpretation can be combined."
It would be indefensible to give everyone an electrocardiogram to screen everyone who might have a heart attack one 24-hour interval.
On the other hand, in certain clinical contexts or on the basis of specific evocative symptoms, at that place, yes, an electrocardiogram can be benign.
Back toRT-PCR and Ct (Cycle Time or Cycle Threshold).
In the case of an infectious disease, peculiarly a viral i, the notion ofcontagiousness is another important chemical element.
Since some scientific circles consider that an asymptomatic person tin transmit the virus, they believe information technology is important to test for the presence of virus, even if the person is asymptomatic, thus extending the indication of RT-PCR to everyone.
Are RT-PCR tests proficient tests for contagiousness?
This question brings united states of america dorsum to the notion of viral load and thereforeCt.
The relationship between contagiousness and viral load is disputed by some people and no formal proof, to date, allows us to make a decision.
All the same, common sense gives obvious credence to the notion that the more virus a person has inside him or her, especially in the upper airways (oropharynx and nasopharynx), with symptoms such as coughing and sneezing,the higher the risk of contagiousness, proportional to the viral load and the importance of the person's symptoms.
This is calledcommon sense, and although modern medicine has benefited greatly from the contribution of science through statistics and Evidence-Based Medicine (EBM), it is still based primarily on common sense, feel and empiricism.
Medicine is theart of healing.
No examination measures the amount of virus in the sample!
RT-PCR isqualitative: positive (presence of the virus) or negative (absenteeism of the virus).
This notion of quantity, therefore of viral load, can be estimated indirectly by the number of amplification cycles (Ct) used to highlight the virus sought.
-
The lower the Ct used to discover the virus fragment, the college the viral load is considered to be (loftier).
-
The higher the Ct used to detect the virus fragment, the lower the viral load is considered to be (low).
Thus, the French National Reference Centre (CNR), in the acute phase of the pandemic, estimated that the peak of viral shedding occurred at the onset of symptoms, with an amount of virus corresponding toapproximately 108 (100 meg) copies of SARS-CoV-2 viral RNA on average (French COVID-19 cohort data) with a variable duration of shedding in the upper airways (from 5 days to more than v weeks) [19].
This number of 108 (100 million) copies/μl corresponds to a very depression Ct.
A Ct of 32 corresponds to ten-15 copies/μl.
A Ct of 35 corresponds to about 1 copy/μl.
To a higher place Ct 35, information technology becomes incommunicable to isolate a complete virus sequence and culture information technology!
In French republic and in most countries, Ct levels above 35, even 40, are still used fifty-fifty today!
The French Order of Microbiology (SFM) issued an opinion on September 25, 2022 in which it does not recommend quantitative results, and it recommends to make positive upwardly to a Ct of 37 for a single gene [20]!
With ane copy/μl of a sample (Ct 35), without cough, without symptoms, one tin sympathize why all these doctors and scientists say thata positive RT-PCR examination means naught, nothing at all in terms of medicine and dispensary!
Positive RT-PCR tests, without any mention of Ct or its relation to the presence or absence of symptoms, are used as is past our governments as the exclusive statement to apply and justify their policy of severity, austerity, isolation and aggression of our freedoms, with the impossibility to travel, to meet, to alive normally!
There is no medical justification for these decisions, for these governmental choices!
In an commodity published on the website of the New York Times (NYT) on Saturday, August 29, American experts from Harvard University are surprised that RT-PCR tests as practiced can serve every bit tests of contagiousness, even more so equally evidence of pandemic progression in the instance of SARS-CoV-ii infection [21].
According to them, the threshold (Ct) considered results in positive diagnoses in people who do not represent any chance of transmitting the virus!
The binary "yes/no" answer is not enough, according to this epidemiologist from the Harvard University School of Public Wellness.
"It's theamount of virus that should dictate the course of activeness for each patient tested. »
The corporeality of virus (viral load); just also and above all the clinical state, symptomatic or non of the person!
This calls into question the utilize of the binary result of this RT-PCR test tomake up one's mind whether a person is contagious and must follow strict isolation measures.
These questions are being raised by many physicians effectually the world, non only in the Usa but likewise in France, Kingdom of belgium (Kingdom of belgium Wellness Experts Demand Investigation Of WHO For Faking Coronavirus Pandemic), France, Germany, Italia, the United Kingdom, the United states and the United Kingdom. in Germany, Spain…
Co-ordinate to them:
"We are going to put tens of thousands of people in confinement, in isolation, for goose egg. » [22]. 22] And inflict suffering, anguish, economical and psychological dramas by the thousands!
Nearly RT-PCR tests set the Ct at forty, according to the NYT. Some set up it at 37.
"Tests with such loftier thresholds (Ct) may not merely detect alive virus but also cistron fragments, remnants of an old infection that do not represent any item danger," the experts said.
A virologist at the University of California admits that an RT-PCR test with a Ct greater than 35 is too sensitive. "A more than reasonable threshold would be between 30 and 35," she adds.
Almost no laboratory specifies the Ct (number of amplification cycles performed) or the number of copies of viral RNA per sample μl.
Here is an case of a laboratory upshot (approved by Sciensano, the Belgian national reference middle) in an RT-PCR negative patient:
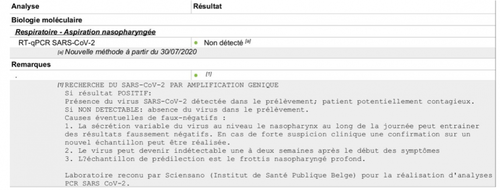
No mention of Ct.
In the NYT, experts compiled three datasets with officials from u.s. of Massachusetts, New York and Nevada that mention them.
Conclusion?
"Up to 90% of the people who tested positive did not carry a virus. »
The Wadworth Center, a New York Country laboratory, analyzed the results of its July tests at the request of the NYT: 794 positive tests with a Ct of 40.
"With aCt threshold of 35, approximatelyhalf of these PCR tests would no longer exist considered positive," said the NYT.
"And aboutlxx% would no longer exist considered positive with aCt of 30! "
In Massachusetts,between 85 and 90% of people who tested positive in July with a Ct of 40 would take been considerednegative with a Ct of 30, adds the NYT.And yet, all these people had to isolate themselves, with all the dramatic psychological and economic consequences, while they were not sick and probably not contagious at all.
In France, the Centre National de Référence (CNR), the French Social club of Microbiology (SFM) continue to push Ct to 37 and recommend to laboratories to use only one gene of the virus every bit a primer.
I remind you that from Ct 32 onwards, it becomes very difficult to culture the virus or to excerpt a complete sequence, which shows the completely artificial nature of this positivity of the test, with such loftier Ct levels, to a higher place 30.
Similar results were reported by researchers from the Great britain Public Health Agency in an article published on Baronial xiii in Eurosurveillance: "The probability of culturing the virus drops to 8% in samples with Ct levels higher up 35."
In addition, currently, the National Reference Centre in French republic simply evaluates the sensitivity of commercially available reagent kits, not their specificity: serious doubts persist about the possibility of cross-reactivity with viruses other than SARS-CoV-2, such as other beneficial common cold coronaviruses.
Information technology is potentially the same situation in other countries, including Belgium.
Similarly, mutations in the virus may have invalidated certain primers (genes) used to notice SARS-CoV-2: the manufacturers give no guarantees on this, and if the AFP fast-checking journalists tell you lot otherwise, examination their good faith by asking for these guarantees, these proofs.
If they have nothing to hibernate and if what I say is simulated, this guarantee will be provided to you and will prove their expert faith.
-
We must need that the RT-PCR results be returned mentioning theCt used because beyond Ct 30, a positive RT-PCR examination means nothing.
-
We must listen to the scientists and doctors, specialists, virologists who recommend the use ofadapted Ct, lower, at 30. An alternative is to obtain the number of copies of viral RNA/μl or /ml sample.
-
We need togo back to the patient, to the person, to his or her clinical status (presence or absence of symptoms) and from there to judge the appropriateness of testing and the all-time way to translate the result.
Until there is a better rationale for PCR screening, with a known and appropriate Ct threshold, an asymptomatic person should not be tested in any way.
Even a symptomatic person should not automatically be tested, as long as they can place themselves in isolation for 7 days.
Permit's cease this debauchery of RT-PCR testing at too high Ct levels and return to clinical, quality medicine.
In one case nosotros understand how RT-PCR testing works, it becomes impossible to permit the current regime routine screening strategy, inexplicably supported by the virologists in the safety councils, continue.
My hope is that,finally, properly informed, more and more people volition demand that this strategy be stopped, considering it is all of united states of america, enlightened, guided by existent benevolence and mutual sense, who must decide our collective and private destinies.
No ane else should practise information technology for us, peculiarly when we realize that those who decide are no longer reasonable or rational.
Summary of important points :
-
The RT-PCR test is a laboratory diagnostic technique that is not well suited to clinical medicine.
-
It is a binary, qualitative diagnostic technique that confirms (positive test) or not (negative test) the presence of an element in the medium being analyzed. In the case of SARS-CoV-ii, the chemical element is a fragment of the viral genome, not the virus itself.
-
In medicine, even in an epidemic or pandemic situation, information technology is dangerous to place tests, examinations, techniques above clinical evaluation (symptoms, signs). It is the opposite that guarantees quality medicine.
-
The primary limitation (weakness) of the RT-PCR examination, in the current pandemic situation, is its extreme sensitivity (false positive) if a suitable threshold of positivity (Ct) is not called. Today, experts recommend using a maximum Ct threshold of 30.
-
This Ct threshold must exist informed with the positive RT-PCR effect so that the physician knows how to interpret this positive event, especially in an asymptomatic person, in guild to avoid unnecessary isolation, quarantine, psychological trauma.
-
In addition to mentioning the Ct used, laboratories must continue to ensure the specificity of their detection kits for SARS-CoV-2, taking into account its well-nigh recent mutations, and must go on to utilize three genes from the viral genome being studied as primers or, if not, mention it.
Overall Conclusion
Is the obstinacy of governments to use the current disastrous strategy, systematic screening by RT-PCR, due to ignorance?
Is information technology due to stupidity?
To a kind of cerebral trap trapping their ego?
In any case, we should be able to question them, and if amid the readers of this article there are still honest journalists, or naive politicians, or people who have the possibility to question our rulers, then do so, using these clear and scientific arguments.
Information technology is all the more incomprehensible that our rulers have surrounded themselves with some of the most experienced specialists in these matters.
If I have been able to assemble this information myself, shared, I remind you, by competent people above all suspicion of conspiracy, such as Hélène Banoun, Pierre Sonigo, Jean-François Toussaint, Christophe De Brouwer, whose intelligence, intellectual honesty and legitimacy cannot be questioned, and so the Belgian, French and Quebec scientific advisors, etc., know all this besides.
So?
What's going on?
Why continue in this distorted management, obstinately making mistakes?
It is not insignificant to reimpose confinements, curfews, quarantines, reduced social bubbles, to shake up again our shaky economies, to plunge entire families into precariousness, to sow so much fear and anxiety generating a real state of post-traumatic stress worldwide, to reduce access to intendance for other pathologies that still reduce life expectancy much more than COVID-xix!
Is there intent to harm?
Is there an intention to utilize the excuse of a pandemic to movement humanity towards an outcome it would otherwise never have accustomed? In any case, not like that!
Would this hypothesis, which modern censors will hasten to label "conspiracy", exist the well-nigh valid caption for all this?
Indeed, if we draw a straight line from the present events, if they are maintained, we could find ourselves once again bars with hundreds, thousands of human beings forced to remain inactive, which, for the professions of catering, entertainment, sales, fairgrounds, itinerants, canvassers, risks beingness catastrophic with bankruptcies, unemployment, depression, suicides by the hundreds of thousands.
The bear on on teaching, on our children, on teaching, on medicine with long planned care, operations, treatments to exist cancelled, postponed, volition be profound and destructive.
"We chance a looming food crisis if activity is not taken chop-chop."
It is time for everyone to come out of this negative trance, this collective hysteria, because famine, poverty, massive unemployment will kill, mow downward many more people than SARS-CoV-2!
Does all this make sense in the face of a disease that is failing, over-diagnosed and misinterpreted by this misuse of overly sensitively calibrated PCR tests?
For many, the continuous wearing of the mask seems to have get a new norm.
Fifty-fifty if information technology is constantly downplayed by some health professionals and fact-checking journalists, other doctors warn of the harmful consequences, both medical and psychological, of this aseptic obsession which, maintained permanently, is in fact an abnormality!
What a hindrance to social relations, which are the truthful foundation of a physically and psychologically healthy humanity!
Some dare to observe all this normal, or a lesser price to pay in the face of the pandemic of positive PCR tests.
Isolation, distancing, masking of the face up, impoverishment of emotional communication, fear of touching and kissing even within families, communities, between relatives…
Spontaneous gestures of daily life hindered and replaced by mechanical and controlled gestures …
Terrified children, kept in permanent fear and guilt…
All this will take a deep, lasting and negative impact on homo organisms, in their physical, mental, emotional and representation of the world and society.
This is not normal!
Nosotros cannot permit our rulers, for whatever reason, organize our collective suicide any longer.
Translated from French by Global Enquiry. Original source: Mondialisation.ca
Dr Pascal Sacré is a doc specialized in critical care, writer and renowned public health annotator, Charleroi, Belgium. He is a Research Associate of the entre for Research on Globalization (CRG)
* * *
Professionals whose references and comments are the basis of this article in its scientific attribute (specially and mainly on RT-PCR):
one) Hélène Banoun
https://www.researchgate.cyberspace/contour/Helene_Banoun
PhD, Pharmacist biologist
Former INSERM Research Officeholder
Former intern at the Paris Hospitals
two) Pierre Sonigo
Virologist
Research Director INSERM, worked at the Pasteur Institute
Heads the Virus Genetics Laboratory in Cochin, Paris.
Participated in 1985 in the sequencing of the AIDS virus.
iii) Christophe De Brouwer
PhD in Public Wellness Scientific discipline
Honorary Professor at the Schoolhouse of Public Wellness at ULB, Belgium
4) Jean-François Toussaint
Doctor, Professor of Physiology at the University of Paris-Descartes
Director of IRMES, Institute for BioMedical Research and Sports Epidemiology
Former member of the High Quango of Public Health
Source: https://www.zerohedge.com/medical/covid-19-rt-pcr-test-how-mislead-all-humanity-accepting-societal-lock-downs
0 Response to "Is There a Machine That Can Test Eyesight With No Input From the Patient"
Post a Comment